Epidemics and pandemics loom large in history. Few have not heard of the Black Death or Spanish Flu, and Covid-19 still affects our lives. Short, two to three-year outbreaks of these diseases kill quickly and in staggering numbers, but what about the diseases that have stuck around throughout history and brought about death in a much slower fashion?
Tuberculosis (TB) represents one disease that humanity has never managed to shake. A devastating illness marked by a cough and wasting of the body, it has infiltrated all corners of the world, killing more than any other microbial pathogen. The 1700s proved no exception, and the level of contagion associated with the disease meant that once it entered a family, it proved hard to eliminate. Sadly, this became the fate of many members in two generations of the Washington and Lewis families and, undoubtedly others who came in close contact with them. In Part I of this examination of TB in the Washington family, we will examine the disease itself.

Brief History of TB
Tuberculosis originated in East Africa, possibly around 3 million years ago, and evolved into our modern strains between 250-1000 years ago. This makes it one of the oldest diseases still in existence. While primarily a disease of the lungs, TB has the potential to infect most tissues and organs. Skeletal deformities caused by certain strains make it identifiable in the archaeological record, which help to date the disease. As humans migrated across the world, they brought the disease with them. Evidence even exists to suggest that TB thrived in parts of the Americas before the arrival of Europeans. Its presence makes it one of the rare diseases that Europeans did not introduce, though encroachment on indigenous groups and confinement of them to specific areas did lead to a rise in cases. Various names have applied to the disease, but in the Western World, the most common historical names include “consumption,” “White Plague,” and “phthisis.”
Highly contagious, the disease could strike anyone, with those living in cramped and unhygienic conditions experiencing a higher risk of infection. Cities, therefore, had more cases than the countryside. However, the true rate of infection for the 1700s remains unknown as the recording of disease cases did not start until the early 1800s. Once this practice got underway, TB ranked as the leading cause of death in places such as Philadelphia, where it accounted for nearly 15% of all deaths in two separate periods (1807-1826: 7,972 deaths or 15.04%; 1831-1840: 6,093 deaths or 14.23%). From statistics such as this, estimates for previous eras can occur with TB likely causing 25% of all deaths in Europe from the 1600s-1800s and similar numbers occurring in North America.
With such a high rate of infection, and its tendency to spread within families, some came to interpret the disease as inherited, while others continued to support the theory of miasma. A more radical thought blamed vampires, leading to several periods of panic in New England during the 1800s. Today, we understand germ theory, but this would not become mainstream until late 1800s and early 1900s—nevertheless, suggestions of TB’s true contagious nature date to at least 1546. German scientist Robert Koch put the debate to rest when he identified Mycobacterium tuberculosis as the causative agent behind the disease in 1882. The rod-shaped bacteria thus gave the disease its common name. This discovery helped lead to the realization that several strains and forms of the disease exist. While M. tuberculosis spreads via the air and droplets, the zoonotic form of the disease, Mycobacterium bovis, thrives in cattle and their relatives before jumping to humans. This occurs through the consumption of contaminated dairy products and produces a near identical infection to M. tuberculosis.
Despite the pathogen’s deadliness, though also in part of it, TB took on a romantic and fashionable nature. Many a character would suffer from the disease in 19th-century literature, with it running as rampant in the novels of the Brontë sisters as it did in their family, and Lord Byron once lamented his good health since a case of TB would make his appearance more interesting to women. The pale, slim, feverish appearance of the infected fit the ideal female body image that emerged between the late 1700s and mid-1800s. On the extreme end of things, some individuals purposefully exposed themselves to the disease in the hopes of achieving this appearance. A more manageable level saw fashion attempt to mimic the symptoms with corsets and skirts creating the illusion of slim waists while makeup lightened the skin and tinted the cheeks.
Sickness
As with every disease, the onset, severity, and progress of the infection varies depending on the health of the infected individual. For instance, tuberculosis could burn through very young children before anyone identified the disease in the 1700s. Likewise, someone with a stronger immune system might fall ill for a longer period before all the symptoms came to together to provide a diagnosis. Nevertheless, TB has several key identifiers.
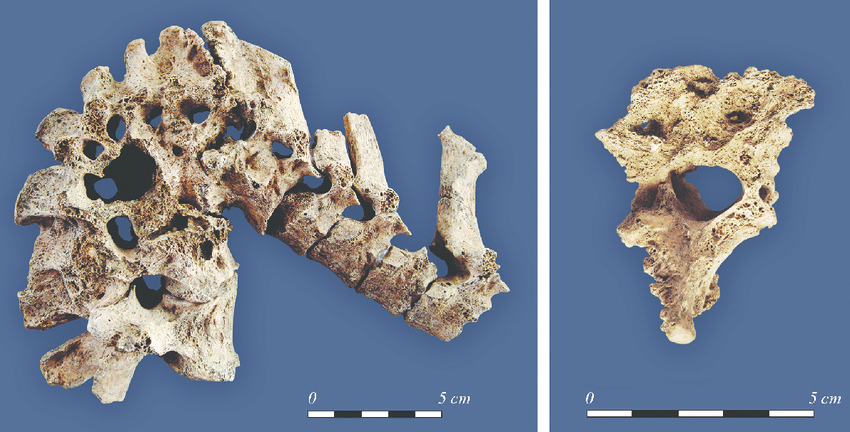
The disease develops in two basic forms, pulmonary and extrapulmonary. The former sees the infection restricted to the lungs and serves as the most common manifestation. Typical symptoms included a cough, which produces blood at a progressed stage, extreme weight loss, decline in appetite, sweats, fever, fatigue, and paleness. The disease can occur over several attacks, interrupted by brief respites, which worsen with time. As the disease progresses, it leaves holes in the lung tissue giving it an appearance akin to Swiss cheese. Extrapulmonary cases pertain to TB that has spread to an organ or tissue outside of the lungs. The standard symptoms remain in addition to physical indications in the impacted areas. This may include enlarged lymph nodes, sores, and spinal deformities that develop over time. Two forms include Pott’s Disease, TB of the spine, and Scrofula, TB of cervical lymph nodes.

While TB can affect all age groups, historically, it has most often struck the young. In Ancient Greece, Hippocrates noted, “phthisis makes its attacks chiefly between the age of eighteen and thirty-five.”1 Higher rates of death amongst those in their twenties and thirties added to the tragedy of the disease, though hope of relief did exist. TB has a unique ability to go dormant during which it walls itself up in the lungs or simply pauses in other parts of the body. While this latent state can reverse at any point, meaning a victim could have years between symptoms and still die of it, the disease may never reactivate. In this scenario, a person would test positive under modern examinations, but suffer no impact to their health or prove contagious to others.
All active cases, however, lead to a decline in the sufferer’s immune system and leaves them open to secondary infections. Cases of pneumonia, as well as meningitis, prove common. A letter from a Fredericksburg woman, dated March 1867, perfectly illustrates the disease. Her son, who had just passed, suffered an “attack of Hemorrhage of the Lungs” first in 1865 and again in “the summer of ’66.” She reported that he recovered from both attacks, but became ill with the mumps in February of 1867 followed by “the symptoms of fell consumption being clearly developed.”2 The boy ultimately lost the strength to rise and found himself confined to a makeshift bed a few months prior to his death.
Treatment
No cure or successful management plan for tuberculosis existed in the 1700s. As such, roughly 66% of cases resulted in death within the first five years of infection. However, lack of success did not stop doctors from prescribing a standard course of treatment that originated in ancient times. To anyone familiar with medical practices of the eighteenth century, the use of emetics, such as mercury and bloodletting, will come as no surprise. Both treatments aimed to purge the body of an affliction, and doctors applied this to nearly every ailment. In truth, these “cure all’s” did more harm than good, with mercury poisoning the patient and bloodletting weakening them. Still, other prescription medicines may have brought some symptomatic relief or, at the very least, not harmed the patient further.
Other forms of treatment involved lifestyle changes in the form of diet and exercise. Viewing items such as meat and alcohol as harmful in large quantities or too difficult for the body to process, doctors instructed TB patients to eliminate them from their diet. Instead, they should consume plenty of milk, preferably from a donkey, and vegetables. On top of this, the patient should increase fast-paced exercise or travel, such as horse riding, to the extent that their strength allowed. This would ideally force clean air into the lungs. While well-intentioned, neither change could treat a bacterial infection.
Other changes involved relocation. Some may be familiar with the phrase “taking the waters” The belief that natural springs, particularly hot ones, provide health benefits dates to prehistory and exists in multiple cultures. Some truth lies in this, but no spring could cure TB beyond the warm waters and steam providing some relief to a weakened, cough-ridden body. Nevertheless, doctors frequently instructed patients to visit springs, giving rise to Berkeley Springs in Colonial Virginia. A destination for wealthy Virginians starting in the mid-1700s, some visited for general health benefits and the social scene, while others went specifically for TB. If none of these treatments worked, doctors would prescribe a course of action that everyone knew served as a last resort: relocating to a warmer climate. In Colonial America, some patients went to the southern colonies while others elected to try the Caribbean (Figure 6). They found no cure in these locations, but the belief in springs and warmer or dryer climates providing relief for TB victims would continue into the 1900s.


Bane of the Washingtons
All forms of tuberculosis mentioned above existed in the 1700s, but which one did the Washingtons have? Parts II & III of our Tuberculosis Blog will closely examine individuals connected to the Washington and Lewis families that had the disease, but we can make a few conclusions. Regarding contraction of the disease, the number of people afflicted, and their close relations to one another, it remains highly probable that they passed it to each other. Of the eight people identified across two generations, none developed a spinal deformity, and no mention of enlarged lymph nodes appear. This implicates pulmonary TB as the likely suspect in all cases.
Nevertheless, we cannot forget M. bovis. With no knowledge of the disease or methods of pasteurization, the frequent consumption of dairy products and presence of cows on farms made it a key source of potential exposure. The Probate Inventory taken in 1743 after Augustine’s death records an inactive dairy building at Ferry Farm. Whether the Washingtons ever used it for dairy remains unknown, but they certainly obtained and consumed dairy products regularly. We will never know what vector the disease took in entering the Washington Family or when each individual first contracted it, but we can piece together how it affected their lives and ultimately ended them. Stay tuned for Parts II and III: The Victims.
Emma Schlauder
Research Archaeologist
Bibliography
Barberis, Ilaria, Nicola Bragazzi, Lucia Galluzzo, & Mariano Martini 2017 The History of Tuberculosis: From the First Historical Records to the Isolation of Koch’s Bacillus. Journal of Preventive Medicine and Hygiene 58: 9-12.
Brown, Kathleen M. 2009 Foul Bodies: Cleanliness in Early America. Yale University Press, New Haven, CT.
Buchan, William 1772 Domestic medicine; or, The family physician: being an attempt to render the medical art more generally useful, by shewing people what is in their own power both with respect to the prevention and cure of diseases. Chiefly calculated to recommend a proper attention to regimen and simple medicines. Evans Early American Imprint Collection, University of Michigan < https://quod.lib.umich.edu/cgi/t/text/text-idx?c=evans;cc=evans;q1=Gout;rgn=main;view=text; idno=N09695.0001.001>. Accessed 11 April 2023.
CDC History of World TB Day. CDC < https://www.cdc.gov/tb/worldtbday/history.htm#:~:text= Johann%20Schonlein%20coined%20the%20term,%E2%80%9Cschachepheth%E2%80%9D%20in%20ancient%20Hebrew.>. Accessed 11 April 2023.
CDC Symptoms of Pulmonary and Extrapulmonary TB Disease. The Division of Tuberculosis Elimination, CDC < https://www.cdc.gov/tb/webcourses/Course/chapter4/4_ diagnosis_of_tb_ disease_4_clinical_practices_symptoms_of_pulmonary_and_extrapulmonary_tb_disease.html>. Accessed 11 April 2023.
2 Conway, Mary Catherine Washington Henry 1867 “Letter to Jane ?, Cabin Mill – March 22, 1867.” Access granted by Suzanne Leigh Peake (owner) and Wyatt Falcone,
1 Daniel, Thomas M. 2006 The History of Tuberculosis. Respiratory Medicine 100: 1862-1870.
Mackowiak, Philip A., Vera Tiesler Blos, Manuel Aguilar, & Jane E. Buikstra 2005 On the Origin of American Tuberculosis. Clinical Infectious Diseases 41(4): 515-518.
Mullin, Emily 2016 How Tuberculosis Shaped Victorian Fashion. Smithsonian Magazine, Smithsonian < https://www.smithsonianmag.com/science-nature/how-tuberculosis-shaped-victorian-fashion-180959029/>. Accessed 11 April 2023.
Nardell, Edward A. 2022 Extrapulmonary Tuberculosis (TB). Merck Manual < https://www.merckmanuals.com/ professional/infectious-diseases/mycobacteria/extrapulmonary-tuberculosis-tb>. Accessed 11 April 2023.
National Jewish Health 2013 Tuberculosis: History. National Jewish Health < https://www.nationaljewish.org/ conditions /tuberculosis-tb/history>. Accessed 11 April 2023.
Otis, Edward O. 1909 The Great White Plague. Thomas Y. Crowell & Co., New York.
Palmer, Mitchell V. 2011 Bovine Tuberculosis and the Establishment of an Eradication Program in the United States: Role of Veterinarians. Veterinary Medicine International.
Rankin-Hill, Lesley M. 1997 A Biohistory of 19th-Century Afro-Americans: The Burial Remains of a Philadelphia Cemetery. Bergin & Garvey, Westport, CT.
White, Tim D., Michael T. Black, & Pieter A. Folkens 2012 Human Osteology, 3rd edition. Elsevier Inc., Burlington, MA.
